7 PRP Treatments That Are Popular Right Now

The time it takes to draw a patient’s blood, add a little citrate, and use a centrifugal machine with a PRP kit is only 15-20 minutes. This is the amount of time needed to create Platelet-Rich Plasma, or PRP. This can then be used for many purposes, using speeding up a patients recovery.
PRP is by far the best healing agent that has growth factors and platelets to help with the healing process, which is also completely free and natural to obtain.
What are The Advantages Of Using PRP Correctly?
It is easy to create PRP simpy by placing blood in a centrifuge, but it can have very little, if any, platelets, and would otherwise be useless. However, with the right equipment, you can make PRP with up to 7x the amount of platelets. This can be amplified by using fat tissue and collagen fibers to create a PRP matrix.
7 Popular PRP Treatments
- Facial Treatments
Many skin centers are thriving due to being one of the first to adopt PRP therapies. With the lack of side effects or down time, it became incredibly popular. These treatments include wrinkle reduction, skin rejuvenation, dark circle and bag erasure, rosacea treatment, and even lip augmentation.
One popular and generic treatment option includes combining PRP and a treatment known as microneedling. When this is applied, it’s effects are similar to facelifts, for far less cost and side effects.
- Hair Loss
PRP growth factors can be beneficial when it comes to reversing non-genetic early stage hair loss. Despite there being a huge market for this, almost no practitioners actually utilize it. Many clients have seen promise after hair thinning, and many have seen beard regrowth over time.
- Arthritis and Cartilage
Arthritis treatments alone cost patients 6.4 billion dollars in 2013 for the US alone, with projections of up to 9 billion by the end of the decade. However, unlike the other treatments, PRP is seen as the only treatment that can not just reduce symptoms, but also regrow the cartilage. One of the most popular examples would be treatments for Temporomandibulaar Joint Osteoarthritis.
- Anti-aging Properties
When it comes to the anti-aging market, there are a endless number of treatments and procures available. Yet, none of them even stand close to the effectiveness of PRP therapy. PRP combined with Microneedling can ve highly effective for strech marks, acne scars, breast augmentation, and even skin conditions like Lichen Sclerosus.
- Pain Relief and Musculoskeletal Healing
There are a ton of treatments in this category, with many of them being incredibly more effective than leading treatments. These include healing Rotator Cuffs, Tennis Elbow, Achilles Tendonitis, Patellar Tendonitis, Back Pain, Hip and Pelvic problems, Degenerative Disc Disease, Golfer’s Elbow, Labaral Tear, Brusitis, neck pain, avascular Necrosis, and even pain related to nerve regeneration.
Almost all of these treatment, as opposed to those in other categories on this list, also use ultrasound guidance when injecting the PRP directly into the affected tissue. This can allow patients to see fantastic results in as little as 2 weeks.
- Fertility
Ovarian Rejuvination is where PRP is injected directly into a woman’s ovaries. This is meant to help reverse menopause and help lower fertility issues. This treatment can even be used for sexual regeneration. Although similar, this treatment is not the same as other treatments where PRO is injected into the vagina, and is supposed to treat looseness, dryness, low sex drive, and incontinence.
- COPD (Chronic Obstructive Pulmonary Disease)
Allergies, asthma, and COPD are among the growing list of things that PRP is being used as a treatment for. For this to work, the PRP is mixed with a saline solution, and then, using a nebulizer, is inhaled, and helps to regenerate the lung tissue.
Although it can take up to 2 months for patients to see the effects, many are seeing improvements. Almost 1 million people suffer from COPD a year, so anything that can help treat the condition is beneficial.
The Future
PRP has been trending rather well in the recent years, and seems to be here for the long term. Not only it is a fully natural remedy, but it is one that works better than most or all traditional treatments. Many like it due to the fact that there are few side effects, it only takes a short amount of time, and there is no recovery period.
PRP has been adopted by thousands of clinics and practices throughout the US and the world. The demand for these treatments have been increasing almost faster than practices are choosing to provide them. Many patients are even willing to travel long distances just to receive these treatments.
So are you providing PRP treatments yet?
- Published in Corporate News / Blog
Why Should you Include PRP In Your Medical Practice?

According to many physicians, PRP (Platelet-Rich Plasma) has been a lifesaver for their practice, while others claimed that it helped them become passionate about medicine again. This is because not only is it 100% from the body of the patient themselves, but it is also natural and comes with pretty much no side effects. It can also be used to treat a plethora of medical ailments, to the point where no other treatment options come close.
Although the above are all fantastic and solid reasons for offering PRP therapies, there are also a couple other reasons as well.
For instance, it is extremely simple compared to other treatment options. For about 1000$ as an initial investment, you can get started with offering PRP. The equipment is relatively cheap, and it pays for itself over a relatively short amount of time.
It also is not just a passing trend, as it has been going popular for a long time and shows no signs of slowing down. The market for PRP therapies is expected to reach almost 500 million dollars within the next 10 years, or an annual growth rate of 12.5% since 2015.
Patient satisfaction is another reason. In certain situations, the satisfaction rate for patients have been as high as 95%. This shocks many of the patients, who believe, although justifiably, that they cannot reverse or halt their condition without side effects, down time, and invasive surgeries.
The time for you to start including PRP into your practice is now, while the supply is low but the demand is booming. There is still a lot more promise when it comes to PRP as well, including combining PRP with other treatments to increase efficacy. Since no standard has yet to be established, you may be starting these standards yourself.
It is vital that we get more doctors to utilize PRP therapy so that they can be a pioneer in this field. PRP can turn medicine on its head, and missing out should not be a smart option.
The best part about it, is that PRP can be utilized in almost every field and specialty, from sports medicine, to pain management, skin rejuvenation, hair care, and even urology. Most of the physicians who utilize this treatment also saw higher patient retention rates as well.
So is there a legitimate reason to not add PRP to your practice?
- Published in Corporate News / Blog
How To Choose A Platelet-Rich Plasma (PRP) Kit

Despite being rather simple, PRP extraction has been shrouded with debate on the reliability of the methods for the past decade. We are going to help clear up the debate by providing information on choosing the best PRP kit.
Using a kit is in itself vital to the creation of PRP. While it is possible to draw blood into a test tube and put it through a centrifuge and claim it is PRP, it’s otherwise ineffective. This is what is known as “bloody PRP,” and it might hold 1.5x the amount of blood platelets if you’re lucky, but it will also contain a ton of red and white blood cells. Because of this, this ineffective form of PRP can potentially cause flare ups after injection.
However, if you use a kit, that concentration of platelets can be as high as 5-7 times the baseline.
What Makes A PRP Kit Good?
This concentration of 5-7 times is vital for PRP to work, and kits allow you to choose whether or not you want to keep in the red and white blood cells, or whether you don’t. Each one would work on different ailments. However, some commercial kits may not deliver what you may want in your PRP, so it is good to know the difference between the kits.
- Gel Separators
Gel separators is pretty much just a test tube with some gel on the bottom. This gel is able to separate the blood from the platelets due to osmosis. The main issue is that when the test tube goes through the centrifuge, most of the platelets will also be caught by the gel as well. This will wind up with 1.5 times concentration of platelets at most, but it does take out the white and red blood cells as well, so that’s a plus.
- Buffy Coat
The kits that allow you to see a buffy coat are most likely to give you concentrations of 5-7 times. A buffy coat is a thin layer that is formed between the blood and the plasma after being in a centrifuge. This is mainly just platelets and white blood cells, with plasma on top, and packed blood underneath.
After this, you have to be able to separate the bufy coat from the red blood cells without contamination. This will help you to get PRP with less than 10% red blood cells.
- Buffy Coat with a Double Spin
The third and final type utilize a buffy coat which is devoid of red blood cells. This is the best kit on the market, because what you do is after separating the PRP from the red blood cells, you spin it again to further get rid of the red blood cells and to concentrate the platelets even more. After this, all that is needed to do is to separate the buffy coat, and this is PRP.
The Biosafe Kit
Although there are many kits that create PRP, the Biosafe kit has to be the best on the market. This is because it give you full control over the end product. Using this machine, you wind up with 10cc of usable product, which you can then double spin for that 5-7 times concentration. You can also choose whether or not you want some red blood cells in the finished product as well.
What is Leukocyte-poor PRP?
Leukocytes are otherwise known as White Blood Cells, and some researchers believe that they can be detrimental to PRP therapy. While there is no consensus as of yet, it is believed by many that these blood cells may trigger an inflammatory response, and even prevent growth factors from creating new cells.
However, some researchers believe that white blood cells are vital to a beneficial response. They believe that without these cells, you will be left with a lot of scar tissue at the site of healing. This Leukocyte-rich PRP also tends to have much more growth factors as well.
If you want to try leukocyte-poor PRP, you will need a Leukocyte Reduction filter, also known as an LR filter. These filters use electrostatic attraction to separate the white blood cells from the rest of the PRP. Although some filters can get clogged, a CIF-LR filter will be able to prevent that and filter out 99.99% of white blood cells.
There Is Plenty Of Evidence To Back This Up
Many people are highly skeptical about PRP, and are willing to ignore it without tons of randomized double-blind studies. Ignoring that some of the things that they do in their practice is also not proven in this manner. Many refuse to even look at the evidence, including the long line of evidence since the 1970’s, ranging over 6000 scientific studies.
The best evidence is how much clients will pay for this despite not being covered by insurance. This shows without any doubt that something about this treatment must be working. As long as there are clients, Adimarket will be there to provide the equipment for practices.
- Published in Corporate News / Blog
Vascular Tissue Engineering: Progress, Challenges, and Clinical Promise
Although the clinical demand for bioengineered blood vessels continues to rise, current options for vascular conduits remain limited. The synergistic combination of emerging advances in tissue fabrication and stem cell engineering promises new strategies for engineering autologous blood vessels that recapitulate not only the mechanical properties of native vessels but also their biological function. Here we explore recent bioengineering advances in creating functional blood macro and microvessels, particularly featuring stem cells as a seed source. We also highlight progress in integrating engineered vascular tissues with the host after implantation as well as the exciting pre-clinical and clinical applications of this technology.
Ischemic diseases, such as atherosclerotic cardiovascular disease (CVD), remain one of the leading causes of mortality and morbidity across the world (GBD 2015 Mortality and Causes of Death Collaborators, 2016, Mozaffarian et al., 2016). These diseases have resulted in an ever-persistent demand for vascular conduits to reconstruct or bypass vascular occlusions and aneurysms. Synthetic grafts for replacing occluded arterial vessels were first introduced in the 1950s following surgical complications associated with harvesting vessels, the frequent shortage of allogeneic grafts, and immunologic rejection of large animal-derived vessels. However, despite advances in pharmacology, materials science, and device fabrication, these synthetic vascular grafts have not significantly decreased the overall mortality and morbidity (Nugent and Edelman, 2003, Prabhakaran et al., 2017). Synthetic grafts continue to exhibit a number of shortcomings that have limited their impact. These shortcomings include low patency rates for small diameter vessels (< 6 mm in diameter), a lack of growth potential for the pediatric population necessitating repeated interventions, and the susceptibility to infection. In addition to grafting, vascular conduits are also needed for clinical situations such as hemodialysis, which involves large volumes of blood that must be withdrawn and circulated back into a patient several times a week for several hours.
In addition to large-scale vessel complications, ischemic diseases also arise at the microvasculature level (< 1 mm in diameter), where replacing upstream arteries would not address the reperfusion needs of downstream tissues (Hausenloy and Yellon, 2013, Krug et al., 1966). Microvascularization has proven to be a critical step during regeneration and wound healing, where the delay of wound perfusion (in diabetic patients, for example) significantly slows down the formation of the granulation tissue and can lead to severe infection and ulceration (Baltzis et al., 2014, Brem and Tomic-Canic, 2007, Randeria et al., 2015).
In order to design advanced grafts, it is important to take structural components of a blood vessel into consideration, as understanding these elements is required for rational biomaterial design and choosing an appropriate cell source. Many of the different blood vessel beds also share some common structural features. Arteries, veins, and capillaries have a tunica intima comprised of endothelial cells (EC), which regulate coagulation, confer selective permeability, and participate in immune cell trafficking (Herbert and Stainier, 2011, Potente et al., 2011). Arteries and veins are further bound by a second layer, the tunica media, which is composed of smooth muscle cells (SMC), collagen, elastin, and proteoglycans, conferring strength to the vessel and acting as effectors of vascular tone. Arterioles and venules, which are smaller caliber equivalents of arteries and veins, are comprised of only a few layers of SMCs, while capillaries, which are the smallest vessels in size, have pericytes abutting the single layer of ECs and basement membrane. Vascular tissue engineering has evolved to generate constructs that incorporate the functionality of these structural layers, withstand physiologic stresses inherent to the cardiovascular system, and promote integration in host tissue without mounting immunologic rejection (Chang and Niklason, 2017).
A suitable cell source is also critical to help impart structural stability and facilitate in vivo integration. Patient-derived autologous cells are one potential cell source that has garnered interest because of their potential to minimize graft rejection. However, isolating and expanding viable primary cells to a therapeutically relevant scale may be limited given that patients with advanced arterial disease likely have cells with reduced growth or regenerative potential. With the advancement of stem cell (SC) technology and gene editing tools such as CRISPR, autologous adult and induced pluripotent stem cells (iPSCs) are emerging as promising alternative sources of ECs and perivascular SMCs that can be incorporated into the engineered vasculature (Chan et al., 2017, Wang et al., 2017).
Importantly, a viable cell source alone is not sufficient for therapeutic efficacy. Although vascular cells can contribute paracrine factors and have regenerative capacity, merely delivering a dispersed mixture of ECs to the host tissue has shown limited success at forming vasculature or integrating with the host vasculature (Chen et al., 2010). Therefore, recent tissue engineering efforts have instead focused on recreating the architecture and the function of the vasculature in vitro before implantation, with the hypothesis that pre-vascularized grafts and tissues enhance integration with the host. In this review, we explore recent advances in fabricating blood vessels of various calibers, from individual arterial vessels to vascular beds comprised of microvessels, and how these efforts facilitate the integration of the implanted vasculature within a host. We also discuss the extent to which SC-derived ECs and SMCs have been incorporated into these engineered tissues.
Clinical Applications
The first reported successful clinical application of TEBV in patients was performed by Shin’oka et al., who implanted a biodegradable construct as a pulmonary conduit in a child with pulmonary atresia and single ventricle anatomy (Shin’oka et al., 2001). The construct was composed of a synthetic polymer mixture of L-lactide and e-caprolactone, and it was reinforced with PGA and seeded with autologous bone marrow-derived mesenchymal stem cells (BM-MSCs). The authors demonstrated patency and patient survival 7 months post-implant, and expanded their study to a series of 23 implanted TEBVs and 19 tissue patch repairs in pediatric patients (Hibino et al., 2010). They were noted to have no graft-related mortality, and four patients required interventions to relieve stenosis at a mean follow-up of 5.8 years. The first sheet-based technology to seed cultured autologous cells, developed by L’Heureux et al., was iterated by the group to induce cultured fibroblast cell sheet over a 10-week maturation period and produce tubules of endogenous ECM over a production time ranging between 6 and 9 months. They dehydrated and provided a living adventitial layer before seeding the constructs with ECs (L’Heureux et al., 2006). Their TEBV, named the Lifeline graft, was implanted in 9 of 10 enrolled patients with end-stage renal disease on hemodialysis and failing access grafts in a clinical trial. Six of the nine surviving patients had patent grafts at 6 months, while the remaining grafts failed due to thrombosis, rejection, and failure (McAllister et al., 2009). An attempt to create an “off the shelf” version of this graft in which pre-fabricated, frozen scaffolds were seeded with autologous endothelium prior to implantation led to 2 of the 3 implanted grafts failing due to stenosis, and one patient passed away due to graft infection (Benrashid et al., 2016).
Most recently, results were reported for the phase II trial of the decellularized engineered vessel Humacyte in end-stage renal disease patients surgically unsuitable for arterio-venous fistula creation (Lawson et al., 2016). This clinical scenario offers a relatively captive patient population in which graft complications are unlikely to be limb or life-threatening, and infectious and thrombotic event rates for traditional materials such as ePTFE are high (Haskal et al., 2010). The manufacturers seeded a 6mm PGA scaffold with SMCs from deceased organ and tissue donors and decellularized the scaffold following ECM production in an incubator coupled with a pulsatile pump prior to implantation. Humacyte demonstrated 63% primary patency at 6 months, 28% at 12 months, and 18% at 18 months post-implant in 60 patients. Ten grafts were abandoned. However, 12-month patency and mean procedure rate of 1.89 per patient-year to restore patency were comparable to PTFE grafts, while higher secondary patency rates were observed (89% versus 55%–65% at 1 year) (Huber et al., 2003, Lok et al., 2013). Although Humacyte revealed no immune sensitization and a lower infection rate than PTFEs (reported up to 12%) (Akoh and Patel, 2010), there remains much work to be done to improve primary patency and reduce the need for interventions.
Harnessing the regenerative functions reported in ECs derived from adult stem cells and iPSCs offers the promise of improving TEBV patency. Mcllhenny et al. generated ECs from adipose-derived stromal cells, transfected them with adenoviral vector carrying the endothelial nitric oxide synthase (eNOS) gene, and seeded the ECs onto decellularized human saphenous vein scaffolds (McIlhenny et al., 2015). They hypothesized that through inhibition of platelet aggregation and adhesion molecule expression, nitric oxide synthesis would prevent thrombotic occlusion in TEBV. Indeed, they reported patency with a non-thrombogenic surface 2 months post-implantation in rabbit aortas. While introducing additional complexities, engineering ECs and SMCs with other regenerative, anti-inflammatory, anti-thrombotic genes could perhaps bridge the functional difference between SC-derived cells and native primary cells.
- Published in Corporate News / Blog
Three popular PRP Treatments for Skincare

Thousands of skincare centers across the nation provide at the very least one kind of PRP treatment. However, most do not go any farther than micro-needling with a topical solution. This is mainly because it is far simpler than all other methods, and it is incredibly popular. However, it would make more sense to many practices who have invested in equipment for add in PRP injections as well.
PRP Is Growing Substantially
Regardless of what is being treated, the protocol for obtaining PRP is the same: You draw the blood, place it in the centrifuge, and then take out the PRP from the rest of the material. This simplicity can be combined with PRP’s vast usability to create significant and mindblowing advances in modern medicine.
This includes skincare as well, as the PRP that you get from patients can be used in a plethora of ways. Here are a couple of examples of what can be performed by dermatologists and plastic surgeons the world over.
- Skin Augmentation
Adding a topical solution of PRP ccombined with microneedling can help to regenerate dying skin cells, and makes skin feel soft. Although this will probably work for most clients, many might want more. For instance, if you want to plump up the face, injecting PRPinto the dermis can help provide both beauty, as well as a healing process.
Although if you want to create volume, you will need a filler. One way to do this is by using a Platelet-Poor Plasma filler, or PPP, which is often left over from the PRP process. You can also use Hyaluronic Adic. A combination of these with PRP have been known to provide wonderful results, with some clinicians boasting a 100% success rate.
- Vitiligo Correction
Many companies will shill out millions of dollars to find out how to turn defective cells healthy again. Many are looking into DNA Technology. However, simply utilizing PRPP may provide the same results. Some studies have shown that adding CO2 laser therapy for correcting vitiligo to a PRP treatment can increase it’s effectiveness by 4 times. This can also be beneficial in other areas, such as correcting wrinkles, and even acne scars. So combining PRP treatments are conventional therapies can boost the effects tremendously.
So if PRP can help boost the effects of lasers, it may be able to also boost the effects of other skin therapies as well. It seems like a great opportunity to continue doing the work that you do, but this time it is more effective due to a simple method. This is something that hundreds of skin care facilities are already providing for their clients.
- Hair Rejuvenation
Mesotherapy is a common treatment that utilizes microinjections that deliver a medication throughout the skin’s service. This prodecure has been able to provide great quality results by adding peptides and vitamins to the mix as well. However, one of the best ways that you can incorporate this into your practice is by using PRP therapy.
Mesotherapy can also be used to provide an even amount of PRP all over the body, including face, neck, hands, etc. This helps to rejuvenate the skin and reduce wrinkles, discoloration, and stretch marks. However, this works best when it comes to hair loss treatments. In fact, adding PRP with mesotherapy has exceeding the expectations that the industry has set.
This is why we think PRP therapy is something that every skincare clinic should offer. Since hair loss effects both men and women, it is important to try to work to make your treatments as effective as possible. Your patients will benefit from it and satisfaction will rise, is there any other reason to put it off?
“But I Never Heard Of Them!”
Some of these treatments and combinations are incredibly new, so new, that many might not have heard of them before. However, this is why signing up to use them as soon as possible is vital. This way, you can bee a step ahead of the competition when it comes to providing great services.
The demand for PRP is only growing over time, and the sooner you can get on board, the better off your practice will be. If you are interested in learning more about PRP therapy, or checking out our line of PRP equipment, you can do so by going to the Adimarket website and checking it out for yourself.
PRP provides more effective treatments for less time, less money, and more satisfaction. Tons off practices have been putting their trust in this treatment and have been reaping the benefits long term. PRP is here to stay, so are you ready to seize the potential of this great medical revolution?,
- Published in Corporate News / Blog
Why Dermatologists Should Use Platelet-Rich Plasma (PRP)

PRP is a powerful means of regenerating tissues, and has pretty a pretty large growth in popularity among patients, especially those who suffer from alopecia. This is despite the apparently lack of evidence that supposedly surrounds the treatment.
Is It A Lack Of Evidence Or Just A Lack Of Funding?The lack of widespread research may have more to do with funding than anything else. Many of the studies that are currently out there about PRP were unfunded, especially on the subject of Hair Regeneration. However, despite this lack of funding, the demand for PRP treatments for hair loss is growing at an unprecedented rate.
When it comes to PRP kits, there are three kinds to choose from. Ones that use gels, one that create a buffy coat, and one that creates a buffy coat utilizing a double spin. It is pretty unanimous that the last option creates the most reliable and concentrated form of PRP possible, at 5-7 times the baseline amount of platelets.
This concentration level also has the most nutrients which helps for the regeneration of blood vessels and stem cells. One commonly recommended tactic is to combine PRP hair regeneration with micro-needling with a topical layer of PRP. This may be beneficial in some cases.
Micro-needling is a way to create small amounts of trauma, which the body reacts to via a healing response. This response, mixed with PRP, can help to stimulate the growth of new cells.
In some instances, a dermatologist might have three sessions, with the first two being PRP injections, and the middle one being a micro-needling with a PRP topical solution. However, micro-needling is completely optional. Whether you choose to use this method or not, you will still be injecting the patient with PRP at the scalp.
Combining PRP with an Allograft Matrix
One thing that many hair regeneration experts do is combine PRP with an Allograft matrix. These are often used when healing wounds, as it changes inactive adult stem cells back into an active form. This makes the wounds heal faster.
This is because an allograft acts like a scaffold that proliferates cell regrowth and speeds up the healing process. Many experts in the fields have noted a high degree of success by using this method.
Allografts are generally made from using the bladder tissue of pigs. However, a better type of allograft is made from amniotic tissues and fluid. This type of allograft can be utilized with little or no chance of being rejected by the body, as opposed to those made from pig bladders.
Medications Vs PRP
The main drugs that are commonly used to regrow hair are Minoxidil and Finasteride. These were designed to be able to prevent male pattern hair loss, but did almost nothing when it came to regrowing lost hair. However, these drugs have been well known to only be temporary solutions, and if the patients stopped taking the drugs, the benefits of them would quickly reverse. These are also not 100% effective at stopping hair loss either, but it can slow the progression.
However, PRP is different. It may actually be the only treatment on the market that has been clinically proven to regrow hair and heal hair follicles. This means that it only only slows down hair loss, but actually helps with hair growth.
Many may ask how temporary the solution is, saying that the other drugs on the market are just temporary solutions. However, many pateints report that a PRP and allograft combination treatment was able to give them great results that lasted for nearly half a decade or more with just one treatment. However, each patient is indeed different.
Aside from drugs, we only had one other choice when it came to hair loss, and that was hair transplants. This is why PRP has been growing in popularity in hair regrowth groups lately. Although those other treatments are not obsolete in the slightest, adding PRP therapy can be both beneficial and safe to patients in the long run.
Some people combine the two, and use PRP alongside Minoxidil and Finasteride with little to no side effects seen to date. You can even combine PRP with laser light scalp stimulation therapy, but that is up to you.
So Try It Out
PRP for hair regeneration, skin rejuvination, and even facelifts is going strong with no sign of stopping. Many dermatologists have already taken the plunge, and since this treatment is not going anywhere anytime soon, it may behoove you to join in on it too.
For more information about PRP including equipment, check out the Adimarket website. We provide great tools for any practice to utilize.
- Published in Corporate News / Blog
Purest Liver-like Cells to Date Generated from Induced Pluripotent Stem Cells (iPSCs)

Researchers from the Medical University of South Carolina (MUSC) and the University of Pennsylvania have discovered a new methodology for purifying liver cells generated from induced pluripotent stem cells (iPSCs) that could facilitate progress toward an important clinical goal: treating patients with disease-causing liver mutations by transplanting unmutated liver cells derived from their own stem cells.
This new technique follows previous attempts to generate liver-like cells from stem cells, which have yielded heterogeneous cell populations with little similarity to diseased livers in patients.
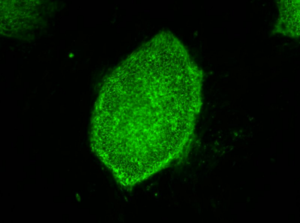
Image: induced pluripotent stem cells expressing a characteristic cell surface protein called SSEA4 (green).
Credit: Image courtesy of Stephen A. Duncan, Ph.D., at the Medical University of South Carolina
The GWAS studies map the genomes in hundreds of people as a way to look for genetic mutation patterns that differ from the genomes of healthy individuals. As GWAS study map more genomes, they become more likely to find the correct genetic mutations that cause a disease. Once a panel of suspected mutations is built, stem cells from these individuals can be manipulated in culture dishes to differentiate into any of the body’s cells. The cells can be screened to learn more about the mutations and to test panels of drugs that might ultimately help treat patients harboring a disease.
Problems arise during the cell manipulation process. For example, iPSCs persistently refuse to mature uniformly into liver-like cells when fed growth factors. Traditionally, antibodies have been used to recognize features of maturity on the surfaces of cells and purify cells that are similar, an approach that has been crucial to stem cell research. But available antibodies that recognize mature liver cells are scanty and tend to recognize many different kinds of cells. The many types of cells in mixed populations have diverse characteristics that can obscure underlying disease-causing genetic variations, which tend to be subtle.
“Without having a pure population of liver cells, it was incredibly difficult to pick up these relatively subtle differences caused by the mutations, but these differences are important in the life of an individual,” Duncan says.
Instead of relying on antibodies, Duncan and his team embraced a new technology called chemo proteomic cell surface capture (CSC) technology. CSC technology allowed the researchers to map the most highly produced proteins on the surface of liver cells during the final stages of differentiation of stem cells into liver cells. The most abundant protein was targeted with an antibody labeled with a fluorescent marker and used to sort the mature liver cells from the rest.
The procedure was highly successful: The team had a population of highly pure, homogeneous and mature liver-like cells. Labeled cells had far more similar traits of mature hepatocytes than unlabeled cells. Pluripotent stem cells that had not differentiated were excluded from the group of labeled cells.
“That’s important,” says Duncan. “If you’re wanting to transplant cells into somebody that has liver disease, you really don’t want to be transplanting pluripotent cells because pluripotent cells form tumors called teratocarcinomas.”
 Duncan cautioned that transplantation of iPSC-derived liver cells is not yet ready for translation to the clinic, but the technology for sorting homogeneous liver cells can be used now to successfully and accurately model and study disease in the cell culture dish.
Duncan cautioned that transplantation of iPSC-derived liver cells is not yet ready for translation to the clinic, but the technology for sorting homogeneous liver cells can be used now to successfully and accurately model and study disease in the cell culture dish.“We think that the ability to generate pure populations will get rid of the variability, and therefore really help us combine with GWAS studies to identify allelic variations that are causative of a disease, at least in the liver,” he says.
Researchers at the University of Minnesota (Minneapolis) and the Medical College of Wisconsin (Milwaukee) contributed to the study, published August 25, in Stem Cell Reports.
###
- Published in Corporate News / Blog
Global Stem Cells Group Plans Bone Marrow Clinical Trials for Knee Osteoarthritis

Global Stem Cells Group has announced plans to hold clinical trials, pending IRB approval, for bone marrow stem cell treatments targeting knee osteoarthritis. The trials will be held in five GSCG facilities in the U.S. and South America, with 25 patients accepted for each location.
MIAMI, March 31, 2016—Pending Institutional Review Board (IRB) approval, Global Stem Cells Group, Inc. has announced plans to conduct a multi-center, placebo controlled clinical trial to measure the safety and effectiveness of the intra-articular application of freshly isolated bone marrow stem cells for the treatment of osteoarthritis.
The clinical trials, which will begin July 1, 2016 and run for one year, will be held in Global Stem Cell Group facilities in Buenos Aires, Argentina; Bogota, Colombia; Quito, Ecuador; Miami, Florida and Topeka, Kansas. Each center will accept 25 patients per clinical trial, and patients will receive a bone marrow stem cell injection in one knee and a placebo in the other knee..
 The trials are designed to investigate the possible beneficial effect of freshly harvested bone marrow stem cell applications on knee osteoarthritis patients in the control group. Patients will receive standard treatment of bone marrow stem cells intravenously, and will be monitored and assessed for any changes in clinical condition.
The trials are designed to investigate the possible beneficial effect of freshly harvested bone marrow stem cell applications on knee osteoarthritis patients in the control group. Patients will receive standard treatment of bone marrow stem cells intravenously, and will be monitored and assessed for any changes in clinical condition.
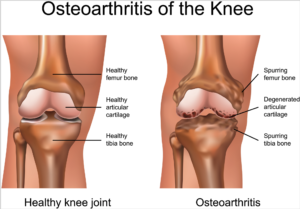
Knee osteoarthritis is a chronic, progressive condition affecting an increasing number of people, especially the elderly and obese. It is characterized by degeneration of the cartilage—the natural cushioning between joints inside the knee.
The condition is the result of the wearing away of cartilage. When this happens, the bones of the joints rub more closely against one another with less of the shock-absorbing benefits of cartilage, resulting in pain, swelling, stiffness and a decreased ability to move.
 According to the Centers for Disease Control (CDC), knee osteoarthritis will affect 67 million people in the United States by 2030. While conventional treatments like physiotherapy or drugs offer temporary relief of clinical symptoms, total knee replacement is the closest treatment available for permanent relief, which requires invasive surgery, comes at a high cost and is not always successful. The latest advances in stem cell therapies for knee osteoarthritis are designed to restore cartilage function in the knee.
According to the Centers for Disease Control (CDC), knee osteoarthritis will affect 67 million people in the United States by 2030. While conventional treatments like physiotherapy or drugs offer temporary relief of clinical symptoms, total knee replacement is the closest treatment available for permanent relief, which requires invasive surgery, comes at a high cost and is not always successful. The latest advances in stem cell therapies for knee osteoarthritis are designed to restore cartilage function in the knee.
Global Stem Cells Group offers the most advanced protocols and techniques in cellular medicine from around the world.
Details of the protocol and eligibility criteria will be released upon IRB approval.
For more information on Global Stems Cell Group, visit the Global Stem Cells Group website, email bnovas(at)stemcellsgroup(dot)com, or call +1 305 560 5337.
About Global Stem Cells Group:
Global Stem Cells Group, Inc, is the parent company of six wholly owned operating companies dedicated entirely to stem cell research, training, products and solutions. Founded in 2012, the company combines dedicated researchers, physician and patient educators and solution providers with the shared goal of meeting the growing worldwide need for leading edge stem cell treatments and solutions. With a singular focus on this exciting new area of medical research, Global Stem Cells Group and its subsidiaries are uniquely positioned to become global leaders in cellular medicine.
Global Stem Cells Group’s corporate mission is to make the promise of stem cell medicine a reality for patients around the world. With each of GSCG’s six operating companies focused on a separate research-based mission, the result is a global network of state-of-the-art stem cell treatments.
To view this press release live online, click here
###
- Published in Press Releases
- 1
- 2