About
Programs
Opportunity
Members
FAQ
News
Blog
About
Programs
Opportunity
Members
FAQ
News
Blog
Stem cell treatment could offer one-end-solution to Diabetes
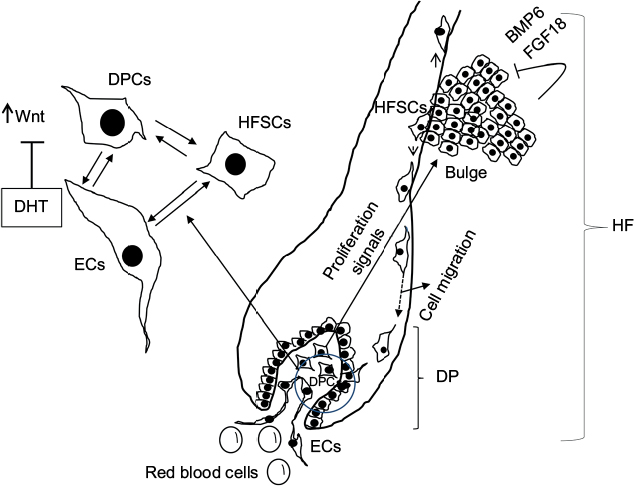
Conventional and novel stem cell based therapies for androgenic alopecia
Menu